
Radiofrequency Ablation
The circuit, the heat, and the lesion

In an era where new energy sources are gaining increasing attention, there is a curious risk in electrophysiology: many professionals use radiofrequency every day, yet few stop to revisit, in depth, how the lesion is actually formed.
Radiofrequency is often treated as something intuitive.
You step on the pedal.
You deliver power.
You watch impedance.
You look for an endpoint.
But radiofrequency is not simply “energy delivered at one point.”
It is a complete electrical circuit, and a lesion is only created when current, resistance, contact, and heat dissipation interact in the expected way. RF energy is delivered in a unipolar fashion, from the catheter tip to the dispersive electrode on the skin, and effective heating occurs because current crosses resistive tissue — not because the generator directly “burns” the myocardium.
So before discussing technique, indices, or strategy, it is worth returning to the most basic question:
what actually happens between the pedal and the myocardium?
1. Radiofrequency is not “energy at the tip.” It is a circuit.
Radiofrequency used in cardiac ablation is a high-frequency alternating current, typically around 500 kHz, delivered in a unipolar fashion from the catheter tip to a dispersive electrode applied to the skin. In other words, lesion formation does not depend on the catheter alone; it depends on the entire circuit.
Current leaves the generator, passes through the catheter, enters the myocardium, travels through the body, and returns via the dispersive patch. The point of highest current density is the catheter-tissue interface because the surface area of the tip electrode is much smaller than the surface area of the dispersive electrode. That difference in area is exactly why useful heating occurs in the heart and not in the skin.
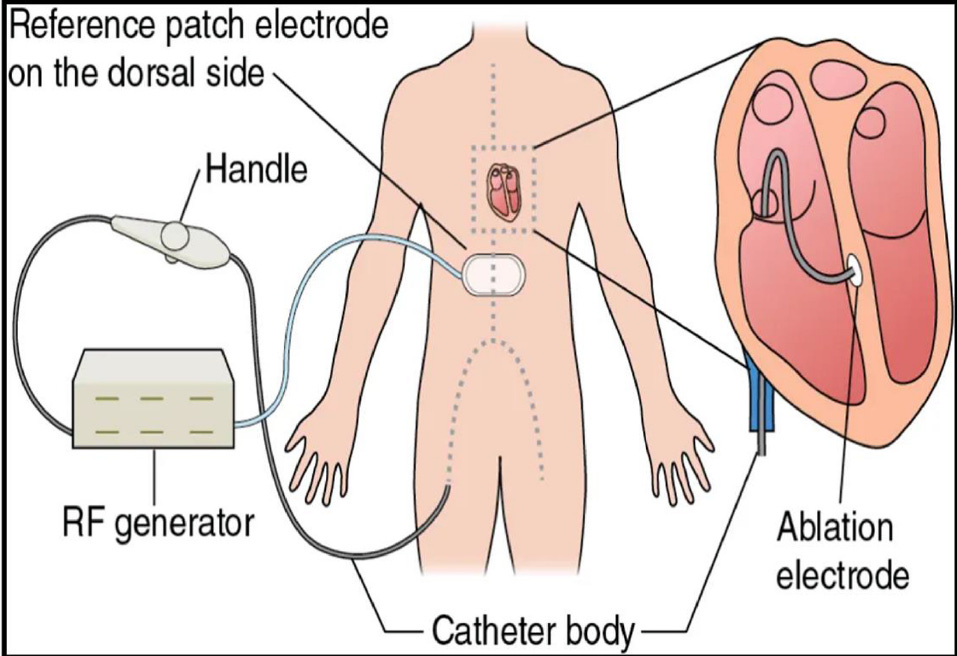
Figure 1 — Unipolar radiofrequency circuit.
Electrical current travels through a complete circuit involving the generator, catheter, myocardium, and dispersive electrode. Lesion formation does not depend only on the catheter tip, but on the behavior of the entire circuit.
Adapted from Patil S, Deshmukh AJ. Biophysics of radiofrequency Ablation: An evolving paradigm. Indian Pacing Electrophysiol J. 2025.
2. How heat is actually produced
When current crosses tissue, it generates local electromagnetic heating — so-called resistive heating. This occurs in the small rim of tissue directly in contact with the electrode. From there, heat propagates into deeper layers through passive thermal conduction, creating a larger zone of conductive heating.
This point is central.
Radiofrequency does not create a homogeneous lesion from the start. First, it directly heats a small superficial rim. Then that energy spreads into deeper tissue. The final lesion depends precisely on the balance between these two phases.
There is also a concept many underestimates: thermal latency. Even after RF delivery stops, tissue temperature may continue to accumulate in deeper layers while the surface interface is already beginning to cool. This helps explain why the final lesion does not always correspond exactly to what seemed to be happening at the surface during the application.
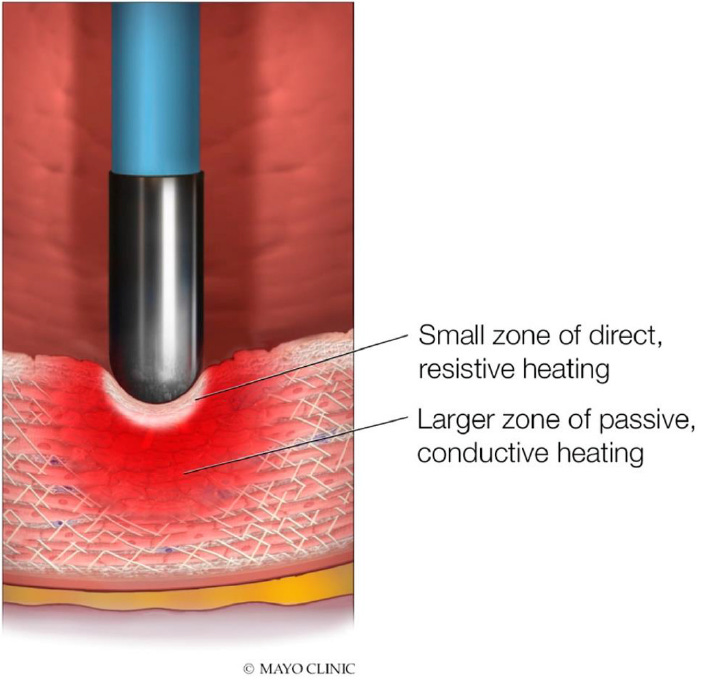
Figure 2 — Resistive and conductive heating.
Radiofrequency produces direct heating in a small superficial zone at the catheter-tissue interface. The lesion then expands in depth through passive thermal conduction.
Adapted from Patil S, Deshmukh AJ. Biophysics of radiofrequency Ablation: An evolving paradigm. Indian Pacing Electrophysiol J. 2025.
3. When tissue becomes non-excitable
Irreversible injury does not occur just because tissue “gets a little warm.”
It occurs when tissue temperature crosses a biological threshold sufficient to produce permanent cellular damage. The article summarizes this thermal continuum well: below 45 °C, excitability is relatively maintained; around 48 °C, reversible loss of excitability may occur; above 50 °C, irreversible tissue injury begins; and at approximately 50.3 °C and 53.6 °C, transient and permanent conduction block appear, respectively.
This matters for two reasons.
First, because acute block is not always equivalent to permanent lesion formation.
Second, because effective RF does not require “boiling” tissue — in fact, once you get too close to that, the problem shifts from inefficacy to complication.
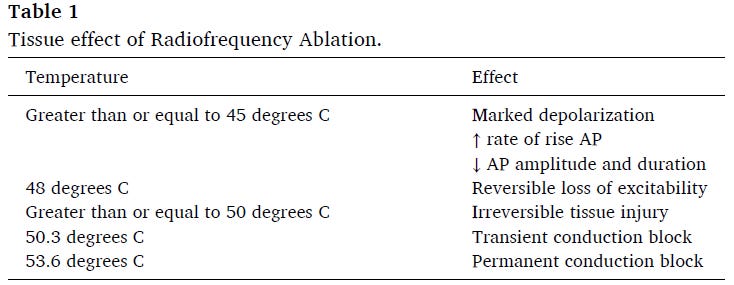
Table 1 — Thermal effects of radiofrequency on tissue.
Excitability, conduction block, and irreversibility of lesion formation depend directly on the temperature reached within the myocardium.
Adapted from Patil S, Deshmukh AJ. Biophysics of radiofrequency Ablation: An evolving paradigm. Indian Pacing Electrophysiol J. 2025.
4. Power is not the lesion
One of the most common conceptual mistakes in the lab is treating power as if it were synonymous with effect.
It is not.
Power is simply the rate of energy delivery per unit time. In the RF circuit, it relates to voltage, current, and resistance. The article summarizes this with the classic relationships: P = V × I and P = I²R, reinforcing that the amount of current actually crossing tissue depends on what the circuit allows.
This changes everything.
Because two applications with the same power may produce different lesions if circuit impedance, tip geometry, or current density differ. The paper provides an elegant example: applications of 20 W at 80 Ω, 30 W at 120 Ω, 40 W at 160 Ω, and 50 W at 200 Ω may result in the same current flow and therefore a similar degree of heating.
So the correct question is not simply “how many watts did I use?” but:
how much current actually entered the tissue, with what density, and under what mechanical and thermal conditions?
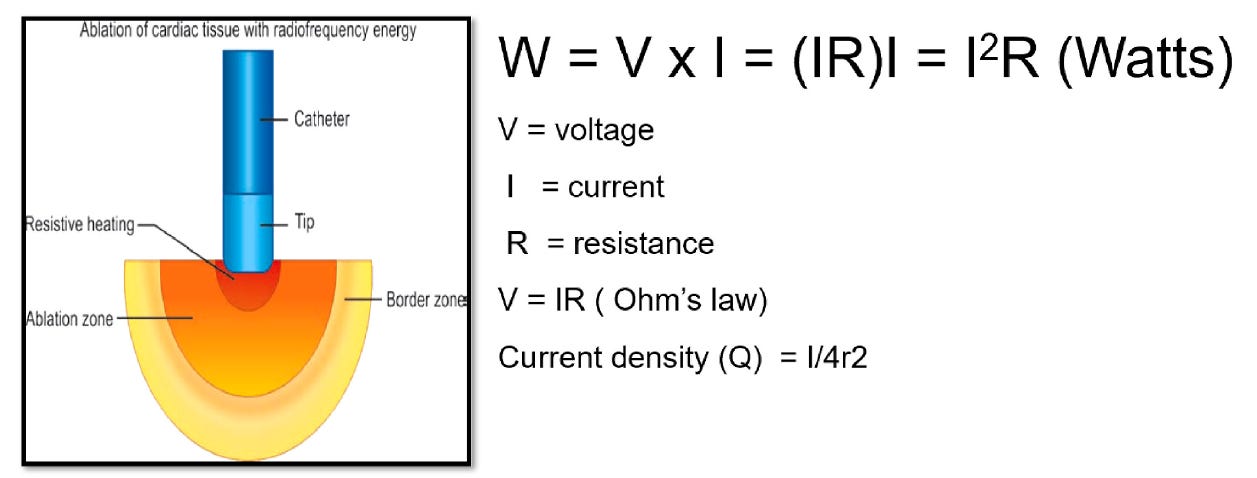
Figure 4 — Power, current, voltage, resistance, and current density.
Lesion formation does not depend only on the power value selected, but on the interaction between power, impedance, and the spatial distribution of current at the catheter-tissue interface.
Adapted from Patil S, Deshmukh AJ. Biophysics of radiofrequency Ablation: An evolving paradigm. Indian Pacing Electrophysiol J. 2025.
5. Why the same power does not create the same lesion
Once the circuit is understood, it becomes easier to see why the same power does not always produce the same lesion.
Lesion size increases with power because more current is delivered to tissue. But that relationship is not absolute. The article emphasizes that larger lesions may occur with higher power, but the risk of overheating at the electrode-tissue interface also rises, and the relationship between power and temperature depends on circuit impedance. This means that applications using the same power can generate different degrees of heating and therefore different lesion dimensions.
Time also changes lesion geometry.
In conventional ablation, most lesion growth occurs within the first seconds, and maximum size is reached as the system approaches thermal equilibrium. The article summarizes this clearly: at constant power, lesion growth occurs mainly in the first 10 seconds and reaches maximal size by about 30 seconds; prolonging beyond that adds little. It also highlights that high-power short-duration tends to produce wider and shallower lesions, whereas lower to moderate power for longer duration favors deeper lesions that depend more on conductive heating.
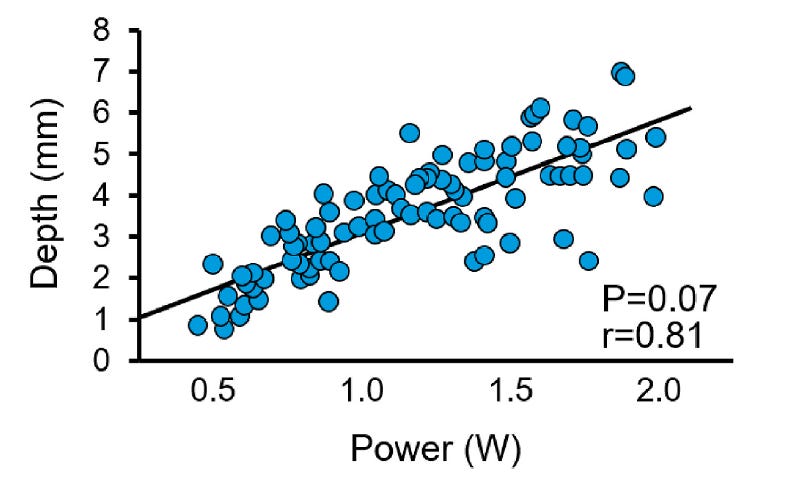
Figure 5 — Relationship between power and lesion depth.
Higher power tends to increase lesion depth and volume, but this effect depends on impedance, time, contact, and heat dissipation.
Adapted from Patil S, Deshmukh AJ. Biophysics of radiofrequency Ablation: An evolving paradigm. Indian Pacing Electrophysiol J. 2025.
6. The dispersive patch is not a detail
Because RF works through a circuit, the dispersive patch is not a logistical accessory. It is a functional part of energy delivery.
The article makes this clear in two ways. First, by explaining that little to no heating occurs at the patch when it has a large surface area and low current density. Second, by warning that poor skin contact, trapped air, sweat, or reduced effective patch area can create focal areas of high current density and skin burns.
This is an excellent practical teaching point, because many people treat the patch as a setup step rather than as a determinant of circuit safety.
In the real world, poor patch adhesion can mean:
higher impedance
less effective current delivery
greater variability in RF application
and, in extreme cases, skin injury
The reasoning is simple: if the small catheter tip acts as a source of high current density, any meaningful reduction in the effective area of the patch moves the system in the wrong direction from a safety perspective.
7. Tip size, current density, and the false intuition of the “larger catheter”
Another concept worth revisiting is the effect of electrode size.
In non-irrigated systems, larger electrodes tolerate higher total power delivery because they dissipate more heat into the blood pool. But that does not mean they will always produce a larger lesion at the same wattage. In fact, the article shows that, at fixed power, an 8 mm tip may produce a smaller lesion than a 4 mm tip because it reduces current density and increases convective heat loss.
In other words:
a larger electrode does not automatically mean a larger lesion.
The effect depends on how much current is actually concentrated at the useful catheter-tissue interface.
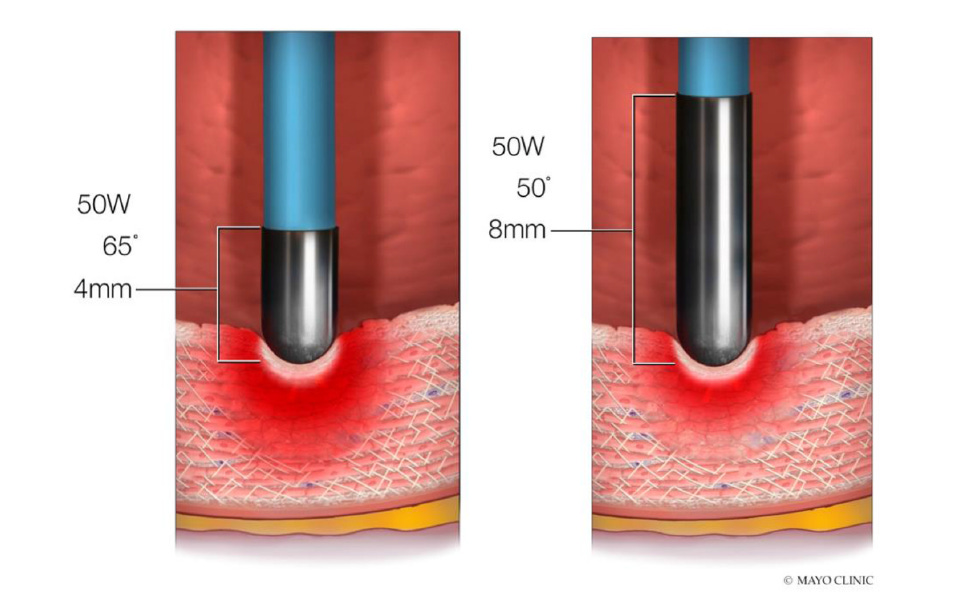
Figure 8 — Effect of tip size on lesion depth.
At the same power, a smaller tip may generate greater current density and a deeper lesion than a larger tip.
Adapted from Patil S, Deshmukh AJ. Biophysics of radiofrequency Ablation: An evolving paradigm. Indian Pacing Electrophysiol J. 2025.
8. Blood flow, irrigation, and heat sink
If heating depended only on power, the problem would be simpler.
But heat does not stay in the tissue.
It is continuously dissipated.
The article highlights two extremely relevant mechanisms of heat loss: convective cooling by circulating blood and the heat sink effect of epicardial vessels. Both reduce effective tissue heating and may limit final lesion size.
This helps explain why certain anatomical regions are more resistant to durable lesion formation even when the application appears adequate.
Irrigation enters exactly at this point. It allows greater power delivery by preventing overheating at the electrode-tissue interface, reducing char formation and enabling larger lesions. In open-irrigated systems, saline cools the tip internally and externally, reducing the risk of coagulum and steam pop. The article also notes that irrigation flow and irrigant composition may alter RF delivery efficiency.
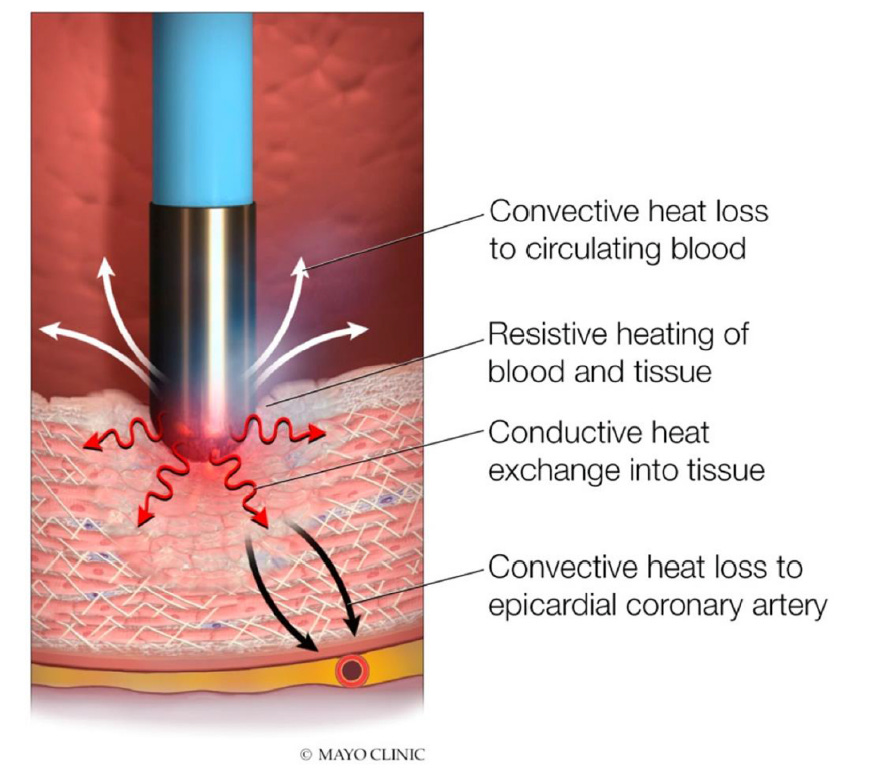
Figure 9 — Convective heat loss and heat sink effect.
Circulating blood and epicardial vessels may dissipate heat and reduce effective lesion depth even when the application appears adequate.
Adapted from Patil S, Deshmukh AJ. Biophysics of radiofrequency Ablation: An evolving paradigm. Indian Pacing Electrophysiol J. 2025.
EP Master Framework
Before stepping on the pedal, think CIRCUIT
Understanding RF biophysics is essential.
But in the lab, knowledge only becomes valuable when it turns into practical reading.
So before each application, it is worth using a simple, repeatable, technically mature framework:
CIRCUIT
Not as a clever word.
But as a way of thinking about RF correctly.
C — Contact
Is the catheter truly supported on tissue, or merely brushing the surface?
Is contact continuous or intermittent?
Does catheter orientation favor real energy delivery, or only the appearance of stability?
Without true contact, there is no efficient resistive heating.
I — Impedance
What is the baseline impedance of this circuit?
Does it make sense for the anatomy, the system, and the intended application?
During RF delivery, is impedance dropping progressively and coherently — or erratically and without meaning?
Impedance is not just a screen detail.
It is an indirect readout of energy transfer.
R — Region
What tissue am I ablating?
Thin atrium, septum, isthmus, ventricular wall, structure near a vessel, region with heat sink effect?
The same power does not mean the same lesion in different regions.
C — Complete circuit
Is the dispersive patch well adhered?
Is irrigation adequate?
Are the generator, cables, and entire circuit functioning as expected?
Radiofrequency does not happen only at the tip.
It depends on the whole circuit.
U — Unit of heat
What type of lesion am I trying to build here?
More superficial? Wider? Deeper?
Power and time only make sense when subordinated to the desired thermal effect.
I — Instability
Is the catheter truly stable or moving on the tissue with respiration or drift?
Is there enough mechanical variation to turn a single application into several incoherent micro-applications?
Instability reduces consistency even when power appears correct.
T — Time
Is application time consistent with the goal, the tissue, and the selected power?
Am I stopping too early, or prolonging beyond the point where lesion gain has already plateaued?
Time is not just duration.
It is depth, thermal conduction, and accumulated risk.
O — Objective
What is the true endpoint of this application?
Block? EGM reduction? Line formation? Substrate modification? Focal elimination?
An application without a clear objective becomes ritual.
And ritual does not create better lesions.
Practical EP Master Box
What elite technicians look at before RF
Elite technicians do not look only at watts.
They mentally check whether:
contact is real
baseline impedance makes sense
the anatomical region supports that strategy
the dispersive patch is correctly positioned and well adhered
catheter stability allows a consistent application
time and power match the lesion objective
In other words:
they do not just observe energy.
They read circuit, tissue, and response.
Conclusion
If I had to summarize everything in one sentence, it would be this:
a radiofrequency lesion is not created by the generator. It is created by the behavior of the circuit inside the tissue.
RF works because current crosses a small interface, generates local resistive heating, propagates heat by conduction, and simultaneously loses heat to blood flow, irrigation, and neighboring structures. The dispersive patch, impedance, tip geometry, contact, and heat dissipation are not details. They are part of the lesion.
So understanding RF is not just understanding how many watts to use.
It is understanding:
how current travels
where heat is generated
where heat is lost
and which variables truly change what happens in the myocardium
That is the foundation.
But foundation alone does not solve the lab.
Because in the real world, the next question is unavoidable:
if I understand the physics, why does the same power still produce such different applications?
That is exactly where the next stage of the series begins.
In the next article, we will move into the most practical and decisive side of radiofrequency:
how to read impedance drop in a useful way
when an application is good and when it only looks good
why contact and stability change everything
how to better interpret overheating risk
and what truly improves lesion quality in daily practice
This will be the first premium article in the series.
Because biophysics explains the lesion.
But correct interpretation of the application is what separates routine from consistency.
EP Master
